|

|
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
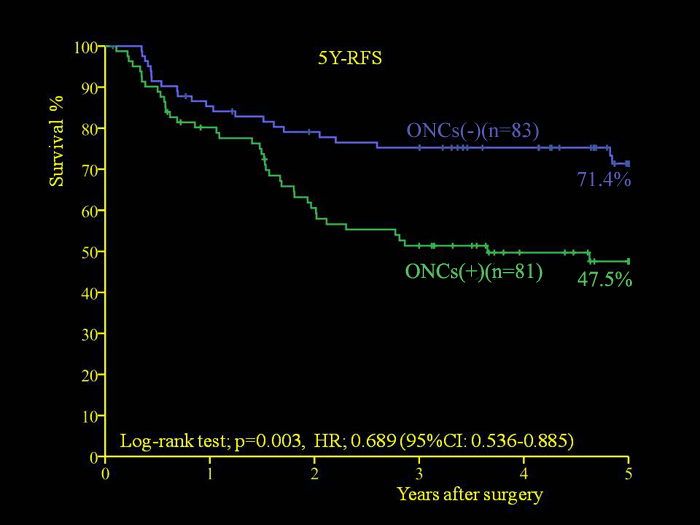
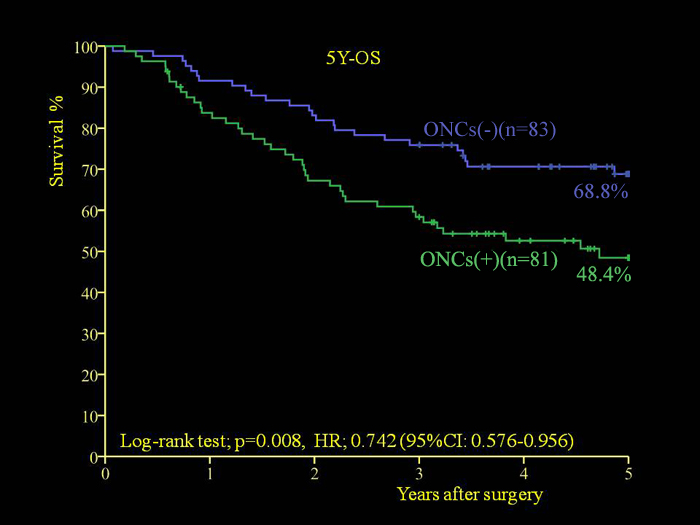
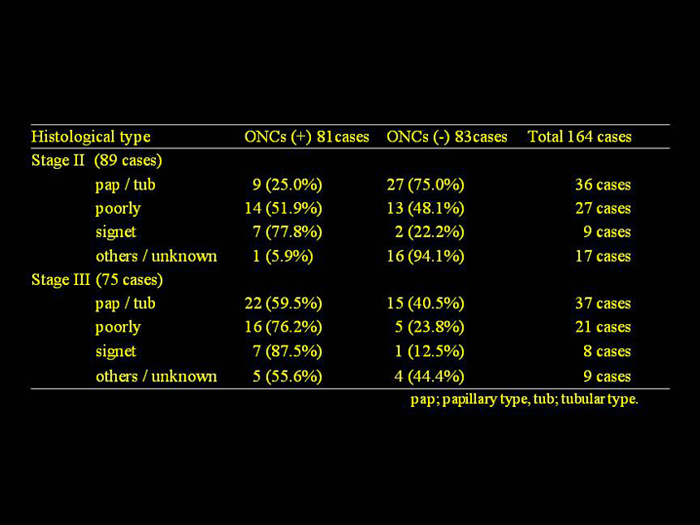
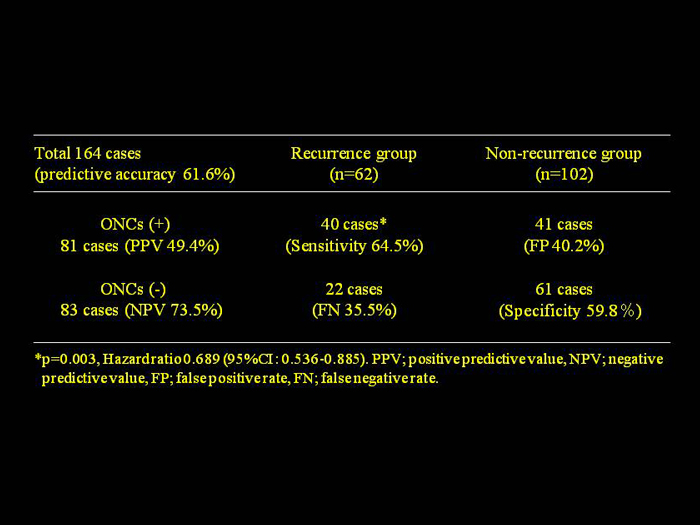
| SEKIDO Y, MUKAI M, KISHIMA K, et al., : Occult neoplastic cells (ONCs) in the lymph node sinuses and recurrence/metastasis of stage II/III gastric cancer. Oncol Letters 2014: In press. |
||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||
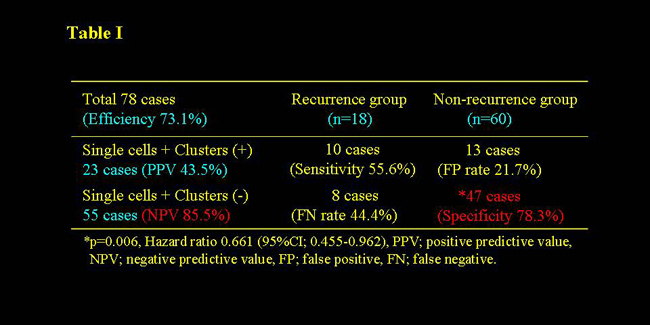
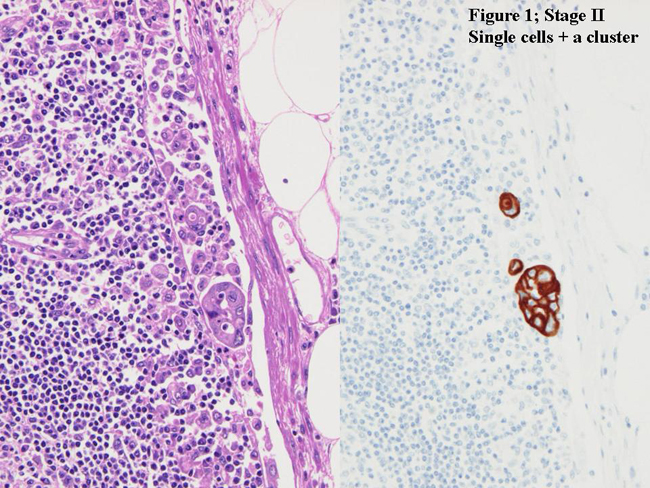
原発性大腸癌のリンパ節にサイトケラチン免疫組織化学染色を行い、Occult neoplastic cells (ONCs)の発現と再発/転移との関連について検討した。Stage II78例, Stage III80例の計158症例を対象とし、3年以内に再発/転移を生じた34例(再発群); Stage II/18例, Stage III/16例と、無再発生存症例124例(無再発群); Stage II/60例, Stage III/64例の2群に分類した。ONCsの発現は1) Single cells type ≧ floating 3-ONCs, 2) Cluster type ≧ floating 1-cluster (2-20 ONCs), 3) Single cells + Cluster typeの3 typeに分類し2群間で比較検討した。Stage II症例のSingle cells typeではSensitivity 55.6% (10/18), Positive predictive value (PPV) 30.3% (10/33), Specificity 61.7% (37/60, p=0.195), Negative predictive value (NPV) 82.2% (37/45)で、Cluster typeではSensitivity 55.6% (10/18), PPV 37.0% (10/27), Specificity 71.7% (43/60, p=0.033), NPV 84.3% (43/51)で、Single cells + Cluster type (Figure 1)では各々55.6% (10/18)/43.5% (10/23), 78.3% (47/60, p=0.006)/85.5% (47/55)であった(Table I)。 |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
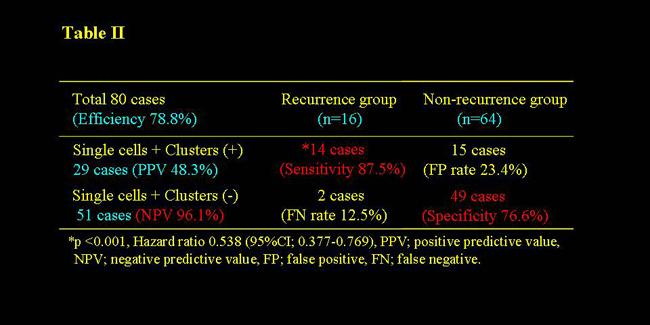
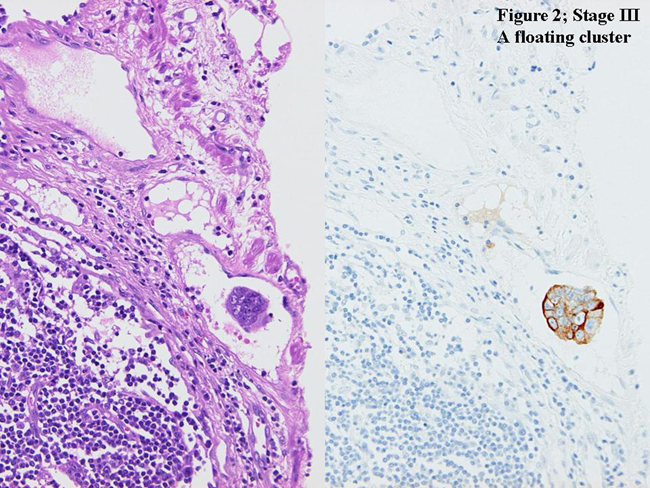
| Stage III症例のSingle cells typeでSensitivity 87.5% (14/16, p=0.002), PPV 32.6% (14/43), Specificity 54.7% (35/64), NPV 94.6% (35/37)で、Cluster type (Figure 2)ではSensitivity 87.5% (14/16, p<0.001), PPV 41.2% (14/34), Specificity 68.8% (44/64), NPV 95.7% (44/46)で、Single cells + Cluster typeでは各々87.5% (14/16, p<0.001)/48.3% (14/29), 76.6% (49/64)/96.1% (49/51)であった(Table II)。 | ||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
| これらの結果より、大腸癌stage II/III症例でONCs; Single cells + Cluster typeが共に発現していない症例は高Specificity/高NPVであり、再発しないと推測される再発低危険群症例が選別可能で、患者の精神的負担軽減やfollow up planに大きく貢献するものと考えられた。さらにStage III症例でONCs; Single cells + Cluster typeの発現症例は高Sensitivityであり、再発すると推測される再発高危険群症例を術後早期に選別可能で、より強力な補助療法が必要であると考えられた。 | ||||||||||||||||||||||||||||||
1) Sekido Y, Mukai M, et al.Occult neoplastic cells in lymph node sinuses and recurrence/metastasis in patients with stage II/Dukes’ B colorectal cancer. Oncol Rep 25: 69-73, 2011. 2) Sekido Y, Mukai M, et al.Occult neoplastic cells in lymph node sinuses and recurrence/metastasis in patients with stage III/Dukes’ C colorectal cancer. Oncol Rep Inpress, 2011. |
||||||||||||||||||||||||||||||
| |
||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||
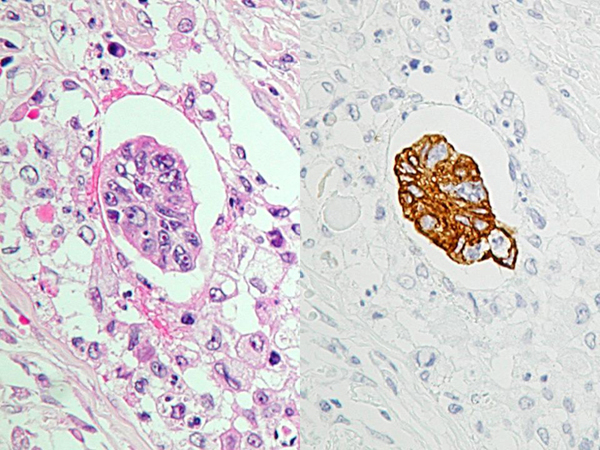
Recurrence and metastasis, cancer cell cluster, occult neoplastic cells (ONCs), colorectal cancer, gastric cancer The photograph shows a cluster of free cancer cells floating in lymph node of a colorectal cancer patient [1]. The cells are positive for cytokeratin on immunohistochemistry (Right: AE1/AE3 stain, ×400). Such clusters exist as a sphere approximately 0.2 mm in diameter or a structure like a bunch of grapes; but it is unknown whether there are interstitial components connecting the individual cancer cells or whether there are special drug-resistant stem cells, which transmit important information, at the center like the queen in a swarm of bees. However, the morphology of these cells and the staining of their cytoplasm and nucleus suggest that the ability to multiply is well maintained. As occult “tumor grafts” floating in lymph or blood, these clusters may have a more important role than single cancer cells in the process of forming micro-metastases in other organs, including the liver and lungs [2,3]. In recent years, methods of genetic and molecular biological analysis have made rapid advances, and these clusters have been studied around the world with respect to inhibition of cell division or reversal of the process of carcinogenesis. To improve the survival of patients, it is important for surgeons who are engaged in treating cancer to manage such tiny tumor cell clusters (approximately 0.2 mm in diameter) during the perioperative period. It is considered most important to eradicate these clusters by dispersing them into single cancer cells with the aid of a “patriot missile” or by inducing a host immune response [4,5]. Is this modern version of Fantastic Voyage nothing but a dream of surgical oncologists? If it becomes possible in the future to visualize tumor cell clusters and their dispersion or dissolution on video, marked improvement of the survival of cancer patients will probably be achieved with no recurrence |
||||||||||||||||||||||||||||||
| |
||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||
|
|